[AHA2011]SATURN试验的临床启示——Steven E. Nissen教授专访
2011 ESC/EAS血脂异常管理指南对LDL-C目标值做出了更严格的要求,如对极高危人群要求将LDL-C降至<70mg/dl或至少降低50%。而只有特定剂量的特定他汀药物才能达到这一目标,如瑞舒伐他汀。多数患者使用强效他汀可以达到<70mg/dl的LDL-C目标值,对极高危患者,这是非常有价值的。
International Circulation: We know that achieving LDLc goals is the primary objective in lipid management. This year’s ESC/EAS Joint Guidelines on dyslipidemia management recommends even lower LDLc goals based on risk stratification. For example, for patients at very high risk, the goal is <70mg/dl or at least a 50% reduction. What should physicians do when they choose statin agents of different LDLc lowering intensities to achieve LDLc goals in their daily practice?
《国际循环》:LDL-C达标是血脂管理的首要目标,今年的ESC/EAS血脂异常管理指南对各危险分层的LDL-C目标值做出了更严格的要求,如,对极高危人群,要求将LDL-C降至<70mg/dl或至少降低50%。在临床实践中,为促使LDL-C达标,医生应如何选择降LDL-C效果不同的他汀类药物?
Dr Nissen: First of all, I agree with the recommendations. If you look at all of the information available across many studies over several decades, the principle that with statins, lowering LDL to lower levels has always produced better outcomes and I do think that for the highest risk patients targeting <70mg/dl is a good goal. What I do and what we recommend is targeting the intensity of statin therapy to what it will take to get to 70mg/dl or less. If a patient starts at 150mg/dl then we are going to need at least a 50% reduction in LDL and only certain doses of certain drugs will get to that level. Most people now, with the very potent statins can get to an LDL of 70mg/dl and in the highest risk patients, this is a very worthy goal.
Dr Nissen: 首先我非常赞同这一建议。综观近些年的大量研究,他汀治疗将LDL-C降至更低水平,均一致显示出更好的结局,因此我认为对极高危患者而言,将LDL-C降至<70mg/dl是更好的目标。我们建议以将LDL-C降至<70mg/dl作为调整他汀治疗强度的标准。如果1例患者的LDL-C基线水平为150 mg/sl,那么我们需要将其降低至少50%,而只有特定剂量的特定他汀药物才能达到这一目标。大多数患者使用强效的他汀可以达到<70mg/dl的LDL-C目标值,对极高危患者,这是非常有价值的。
International Circulation: According to your research, high blood glucose and high blood pressure are related to the progression of atherosclerotic plaques even when LDL is <70mg/dl. Does this suggest that we should aim at even lower LDLc targets against current guidelines in these high risk patients?
《国际循环》:根据您的研究,即使LDL <70mg/dl,高血糖和高血压仍与动脉粥样硬化斑块的进展相关。这是否提示我们,对于这种高危患者应将其LDL-C降至比当前指南要求更低的水平?
Dr Nissen: I think we need the data to make that recommendation. At this meeting we are going to present the SATURN trial, which compared the two most powerful statins in their highest doses – atorvastatin 80 mg and rosuvastatin 40mg. In the atorvastatin arm, we got to an LDL of 70. In the rosuvastatin arm we got to an LDL of 62. There was also a slightly higher HDL with rosuvastatin than with atorvastatin. However, for the primary endpoint, the progression of atherosclerosis, there was statistically no difference between the two regimens. We cannot say at this point that 62 is better than 70 and it was a pretty big study. We would probably need to have more of a difference between the two agents in order to actually see a difference. Interestingly enough in SATURN, for a secondary endpoint and second way of measuring progression by IVUS, there was a difference with a p value of 0.01, so it was highly significant. So it is possible that 60 would be better than 70 but we need more research to answer that question.
Dr Nissen: 我们需要证据以做出这样的推荐。本届大会我们报告了SATURN试验结果。SATURN对比了2种最高剂量的最强效他汀——阿托伐他汀80 mg和瑞舒伐他汀40 mg。结果显示,阿托伐他汀组治疗后LDL-C平均水平为70 mg/dl,而瑞舒伐他汀组达到62 mg/dl;且瑞舒伐他汀组HDL-C也稍高于阿托伐他汀组。然而,试验的主要终点——动脉粥样硬化病变进展,在2组间无统计学差异。这是一项大型研究,基于其结果我们不能说达到62 mg/dl的LDL-C水平比70 mg/dl更好。我们可能需要更多的病例数以显示出2组间的显著差异。SATURN试验中一个有趣的发现是,一项次要终点也是IVUS下检测斑块进展的另一种方法——TAV达到了统计学差异(P<0.01),因此,60 mg/dl的LDL-C水平有可能的确比70 mg/dl更好,但需要更多研究回答这一问题。
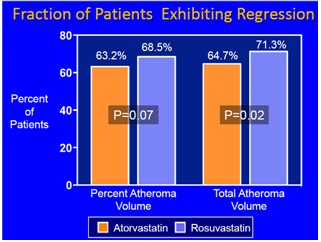
图. 斑块逆转的患者比例
International Circulation: Both high levels of LDLc and low levels of HDLc play key roles in the progression of atherosclerotic plaques. Previous trials like COSMOS and ASTEROID have shown that rosuvastatin can reverse plaques in cardiovascular patients. What do you think is the relationship between the ability of statins to reverse plaque and the intensity of lowering LDLc and raising HDLc levels?
《国际循环》:高LDL-C和低HDL-C在动脉粥样硬化斑块的进展中均发挥重要作用。既往试验如COSMOS和ASTEROID已经显示,瑞舒伐他汀可逆转心血管疾病患者的冠脉斑块。您认为他汀逆转斑块和其降低LDL-C及升高HDL-C的能力有何关联?
Dr Nissen: We have studied this very carefully and it appears that both the degree of LDL reduction and the degree of HDL increase are correlated with the ability to regress disease. In the SATURN trial presented here at this meeting, both drugs atorvastatin in its highest dose and rosuvastatin at its highest dose produced a remarkable degree of regression. In fact, between 65% and 70% of patients on both regimens had less plaque at the end of 24 months than when they began. We have never seen such a large amount of regression in any clinical trial. The reason we saw so much regression is probably because everything else was being very well treated. The patients had very good blood pressure; their diabetes was well controlled in those that were diabetic. What we are seeing in the modern era now is that control of all the risk factors along with optimal treatment of LDL, most patients with coronary disease can actually regress with intensive statin therapy. That is really very good news for patients. Our studies would suggest that it is everything that contributes, not just reduction of LDL levels. If you just treat one risk factor, you don’t get the optimal result.
Dr Nissen: 我们对此进行了细致的研究,结果表明LDL-C降低和HDL-C升高均与他汀逆转病变的能力有关。SATURN试验中,最高剂量的2种他汀均显著逆转了斑块。实际上,65%~70%的患者在24个月随访末期均显示斑块负荷降低。既往任何试验均未观察到如此大比例的病变逆转。这一结果可能是由于各项危险因素都得到了较好的控制,血压水平较理想,糖尿病患者的血糖控制良好。现代研究表明,全面控制危险因素并实现最佳的LDL-C水平,强化他汀治疗的确可以逆转绝大多数患者的冠心病。我们的研究提示,LDL-C水平的降低不是唯一的贡献者。









 京公网安备 11010502033353号
京公网安备 11010502033353号